What is refractory ascites?
What is refractory ascites?
Refractory ascites, that is ascites which cannot be mobilized by low sodium diet and maximal doses of diuretics (up to 400 mg spironolactone or potassium canrenoate and 160 mg furosemide per day), occurs in 5% of cirrhotic patients with ascites.
What causes refractory ascites?
Refractory ascites has a poor prognosis and is associated with complications such as dilutional hyponatremia, hepatorenal syndrome (HRS), spontaneous bacterial empyema (SBEM), hepatic hydrothorax, spontaneous bacterial peritonitis (SBP), and umbilical hernia in the absence of any other precipitating factors3 (Table 2).
What are beta blockers cirrhosis?
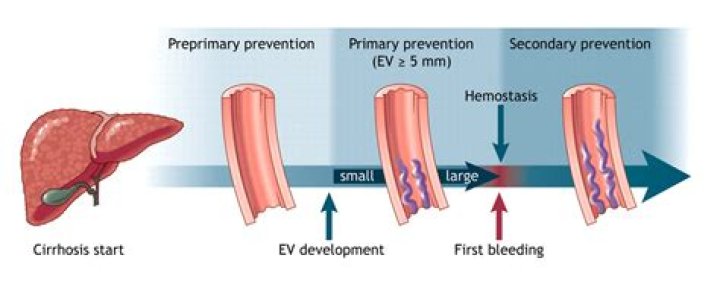
By slowing the heart rate and widening the blood vessels, beta-blocker medicines such as propranolol and nadolol appear to lower the blood pressure in varices that bypass the liver. In people who have esophageal varices, beta-blockers have been shown to reduce the risk of having a first episode of bleeding.
What are the grades of ascites?
The classification of ascites is based on the amount of fluid in the abdominal cavity: grade 1 ascites, or mild ascites, detectable by ultrasound examination; grade 2 ascites, or moderate ascites, characterized by a mild symmetrical abdominal distension; and grade 3 ascites, or large ascites, with significant abdominal …
How is refractory ascites treated?
Therapy for refractory ascites is limited. The available therapies are repeated large volume paracentesis (LVP), transjugular intrahepatic portosystemic shunts, peritoneovenous shunts, investigational medical therapies, and liver transplantation. LVP with concomitant volume expanders is the initial treatment of choice.
What is refractory ascites in liver cirrhosis?
Refractory ascites refers to the inability to respond to medical and dietary management (whether intolerant or unresponsive to diuretics) or rapid reaccumulation of ascites after LVP [37,38].
Are beta blockers bad for the liver?
Drug-induced liver injury is a common cause of acute liver failure. β-blockers are a widely prescribed class of medications; however, hepatotoxicity is a rare adverse effect of this medication of which clinicians must be aware. This case suggests that hepatotoxicity may be a class effect of β-blockers.
When do you stop taking beta blockers for cirrhosis?
As a result, it is recommended that beta blockers be discontinued in patients with cirrhosis with evidence of refractory ascites, systolic blood pressure <90 mm Hg, mean arterial pressure ≤82 mm Hg, serum sodium level <120 mEq/L, acute kidney injury, hepatorenal syndrome, spontaneous bacterial peritonitis, sepsis.
Is ascites the end-stage?
Patients with abnormal liver function who develop ascites, variceal hemorrhage, hepatic encephalopathy, or renal impairment are considered to have end-stage liver disease (ESLD).
What is the best management option for refractory ascites?
Due to the difficulty in receiving a liver transplantation (LT), the ultimate solution for refractory ascites, most cirrhotic patients have selected the palliative therapy such as repeated serial paracentesis, transjugular intrahepatic portosystemic shunt, or peritoneovenous shunt to improve their QOL.